
How to Identify Genetic Causes of Recurrent Pregnancy Loss
Genetic causes of recurrent pregnancy loss (RPL) are chromosomal abnormalities in either parent or embryo that repeatedly disrupt normal fetal development, leading to miscarriage—most commonly balanced translocations, aneuploidy, or single-gene mutations.
Why genetic testing matters after repeated miscarriages
Recurrent pregnancy loss often has a genetic explanation—and identifying it early can dramatically improve the chances of a successful pregnancy.
If you’ve experienced two or more miscarriages, uncertainty becomes overwhelming. Many couples are told to “keep trying,” yet repeated losses may signal a hidden chromosomal issue that standard prenatal care cannot detect. Without targeted testing, the same outcome can repeat again and again.
Recurrent pregnancy loss (RPL) is clinically defined as two or more consecutive miscarriages before 20 weeks of gestation. Research shows that genetic abnormalities account for approximately 50–60% of early pregnancy losses and remain one of the most actionable diagnostic categories in reproductive medicine.
Understanding whether chromosomal rearrangements, embryo aneuploidy, or inherited gene variants are involved allows clinicians to recommend interventions such as parental karyotyping, preimplantation genetic testing (PGT), or targeted fertility strategies. Identifying the genetic cause shifts care from uncertainty to precision.
What is recurrent pregnancy loss and when is genetic testing recommended?
Genetic testing is recommended after two or more consecutive miscarriages, especially when losses occur in the first trimester or there is a family history of chromosomal disorders.
Recurrent pregnancy loss affects approximately 1–2% of couples trying to conceive. While lifestyle, hormonal imbalance, uterine abnormalities, and autoimmune conditions contribute to miscarriage risk, genetic factors remain the leading identifiable cause.
Professional societies such as the American Society for Reproductive Medicine recommend genetic evaluation when:
- Two or more unexplained pregnancy losses occur
- Losses happen before 10–12 weeks gestation
- There is a known chromosomal condition in the family
- Parents have infertility combined with miscarriage history
- A prior fetus showed structural abnormalities
Early genetic evaluation helps avoid unnecessary delays in treatment planning.
Which chromosomal abnormalities cause recurrent pregnancy loss?
Balanced translocations, Robertsonian translocations, inversions, and embryo aneuploidy are the most common chromosomal abnormalities linked to recurrent pregnancy loss.
Chromosomal abnormalities disrupt embryo development by altering gene dosage or structure. Even when parents appear healthy, hidden rearrangements can affect embryo viability.
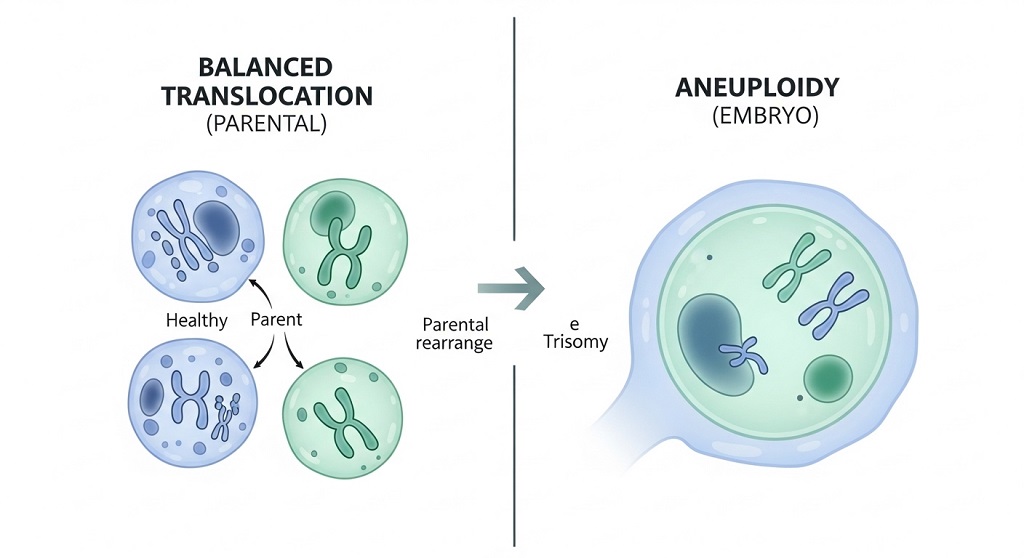
Balanced translocations
Balanced translocations occur when chromosome segments exchange positions without losing genetic material. Carriers are usually asymptomatic but produce embryos with missing or duplicated chromosome segments.
About 2–5% of couples with recurrent miscarriage carry balanced translocations.
Robertsonian translocations
These involve fusion of two acrocentric chromosomes and are associated with miscarriage risk and chromosomal syndromes such as trisomy 13 or trisomy 21.
Chromosomal inversions
Inversions rearrange chromosome segments within the same chromosome. They can disrupt gene expression during embryo development.
Aneuploidy
Aneuploid embryos contain extra or missing chromosomes. This is the most frequent cause of early miscarriage, especially with increasing maternal age.
How does parental karyotyping help diagnose genetic miscarriage risk?
Parental karyotyping detects structural chromosome rearrangements that increase the likelihood of producing nonviable embryos.
Karyotyping analyzes chromosome number and structure using a blood sample from each partner. It identifies translocations, inversions, and mosaicism that routine fertility testing cannot detect.
Testing is particularly useful when:
- Miscarriages occur repeatedly without explanation
- Embryos show chromosomal abnormalities
- There is a family history of genetic disorders
- Previous pregnancies ended in fetal anomalies
If abnormalities are detected, genetic counseling becomes essential for interpreting reproductive risks and options.
What role does embryo genetic testing play in identifying miscarriage causes?
Embryo genetic testing identifies chromosomal abnormalities before implantation, helping determine whether embryo viability is responsible for pregnancy loss.
Preimplantation genetic testing for aneuploidy (PGT-A) screens embryos created through IVF for chromosome errors. This allows clinicians to transfer only chromosomally normal embryos.
Benefits include:
- Reduced miscarriage risk
- Higher implantation success rates
- Improved pregnancy outcomes in older patients
- Better embryo selection accuracy
Studies suggest PGT-A may significantly improve live birth rates among couples with structural chromosomal rearrangements.
Which single-gene disorders contribute to recurrent pregnancy loss?
Single-gene mutations affecting coagulation, immune signaling, or embryonic development can increase miscarriage risk in certain couples.
Although less common than chromosomal abnormalities, monogenic disorders still play a clinically meaningful role.
Examples include:
- Thrombophilia-related gene variants
- Inherited metabolic disorders
- Autosomal recessive developmental syndromes
- X-linked lethal mutations
Carrier screening panels help identify these risks before future pregnancies.
How does maternal age influence genetic miscarriage risk?
Maternal age increases miscarriage risk primarily because older eggs are more likely to contain chromosomal abnormalities.
The probability of embryo aneuploidy rises sharply after age 35. By age 40, more than half of embryos may contain chromosome errors.
| Maternal Age | Estimated Aneuploidy Risk | Miscarriage Risk |
|---|---|---|
| Under 30 | 20–25% | 10–12% |
| 35 | 35–40% | 20% |
| 40 | 50–60% | 40% |
| 42+ | 70%+ | 50%+ |
This is why age-adjusted genetic evaluation is often recommended after recurrent pregnancy loss.
Can genetic counseling improve pregnancy outcomes after recurrent miscarriage?
Genetic counseling helps couples understand test results, recurrence risks, and reproductive options tailored to their genetic profile.
A genetic counselor interprets laboratory findings and explains whether miscarriage risk remains high or manageable. Counseling supports decision-making about IVF, donor gametes, or natural conception strategies.
Typical counseling outcomes include:
- Clarifying recurrence probability
- Selecting appropriate testing pathways
- Evaluating IVF with PGT options
- Planning prenatal diagnostic strategies
What genetic tests are recommended after recurrent pregnancy loss?
Recommended genetic tests include parental karyotyping, embryo testing, carrier screening panels, and products-of-conception analysis after miscarriage.
Each test provides different diagnostic insight.
| Test Type | Purpose | When Used |
|---|---|---|
| Parental karyotyping | Detect chromosome rearrangements | After 2+ miscarriages |
| PGT-A | Screen embryo chromosome number | During IVF cycles |
| Carrier screening | Identify recessive mutations | Before conception |
| POC testing | Analyze miscarriage tissue | After pregnancy loss |
Is recurrent pregnancy loss always genetic?
No, recurrent pregnancy loss is not always genetic—hormonal, anatomical, autoimmune, and lifestyle factors can also contribute.
Common non-genetic causes include:
- Uterine structural abnormalities
- Thyroid dysfunction
- Antiphospholipid syndrome
- Progesterone deficiency
- Uncontrolled diabetes
Because causes often overlap, comprehensive evaluation improves diagnostic accuracy.
How are miscarriage tissue samples used to identify genetic causes?
Testing miscarriage tissue helps determine whether chromosomal abnormalities caused pregnancy loss.
Products-of-conception testing uses microarray analysis or karyotyping to detect missing or extra chromosomes. Identifying aneuploidy confirms that the miscarriage was likely random rather than recurrently inherited.
This information guides future fertility decisions and prevents unnecessary treatment interventions.
What treatment options exist after identifying a genetic cause?

Treatment options depend on the specific genetic diagnosis but may include IVF with PGT, donor gametes, targeted medical therapy, or natural conception with monitoring.
Examples include:
- PGT-SR for translocation carriers
- PGT-A for age-related embryo errors
- Anticoagulation therapy for thrombophilia variants
- Donor egg or sperm when mutation risk is high
Personalized treatment strategies significantly improve live birth probability.
American Society for Reproductive Medicine (.org): What is Recurrent Pregnancy Loss (RPL)? Patient Education Fact Sheet — Establishes the standard definition of RPL and the common known causes.
Conclusion: What is the most effective way to identify genetic causes of recurrent pregnancy loss?
The most effective strategy combines parental karyotyping, embryo genetic testing, miscarriage tissue analysis, and genetic counseling to pinpoint the underlying cause and guide treatment.
Recurrent pregnancy loss is emotionally and medically complex, but modern genetic diagnostics provide clarity in many cases once considered unexplained. Identifying chromosomal rearrangements, embryo aneuploidy, or inherited mutations enables targeted fertility planning rather than repeated uncertainty.
Early testing shortens the path to answers and improves pregnancy outcomes. Couples who pursue structured genetic evaluation often move from repeated loss toward informed reproductive choices.
If recurrent miscarriage has affected your family, consider requesting genetic evaluation early in the diagnostic process. Precision testing transforms guesswork into strategy and increases the chances of a healthy pregnancy.
FAQ: Genetic causes of recurrent pregnancy loss
How common are genetic causes of recurrent miscarriage?
Genetic abnormalities account for roughly half of early pregnancy losses and about 2–5% of recurrent miscarriage cases involving parental chromosomal rearrangements.
Can recurrent pregnancy loss be prevented if it is genetic?
Some genetic causes cannot be prevented but can be managed using IVF with genetic screening, donor gametes, or targeted reproductive planning.
Should both partners undergo genetic testing after miscarriages?
Yes, both partners should be tested because chromosomal rearrangements in either parent can increase miscarriage risk.
Is IVF required if a genetic cause is identified?
Not always; IVF is recommended mainly when embryo screening improves success rates, such as in translocation carriers or age-related aneuploidy risk.
Does one miscarriage mean there is a genetic problem?
No, a single miscarriage is usually random and does not automatically indicate an inherited genetic condition.
Can healthy couples still carry chromosomal abnormalities?
Yes, carriers of balanced chromosomal rearrangements are typically healthy but may produce embryos with genetic imbalances.
When should genetic counseling be scheduled after pregnancy loss?
Genetic counseling is recommended after two consecutive miscarriages or earlier if there is a family history of chromosomal conditions.
Read More Also Boost Your Metabolism After 40 Science-Backed Guide
Discover More: Common signs of hearing loss to know